Spotlight On: Pediatric and Adolescent Gynecology


This month we cast a spotlight on articles, SurgeryU videos, and Journal of Minimally Invasive Gynecology (JMIG) article recommendations from the AAGL Pediatric and Adolescent Gynecology Special Interest Group (SIG) led by Chair, Lissa Yu, MD.
Access to SurgeryU and JMIG are two of the many benefits included in AAGL membership. The SurgeryU library features high-definition surgical videos by experts from around the world. JMIG presents cutting-edge, peer-reviewed research, clinical opinions, and case report articles by the brightest minds in gynecologic surgery.
SurgeryU video and JMIG article recommendations by our SIGs are accessible by AAGL members only. For full access to SurgeryU, JMIG, CME programming, and member-only discounts on meetings, join AAGL today!

It has been a wonderful experience being a part of this AAGL Pediatric and Adolescent Gynecology Special Interest Group (PAG SIG) since its inception five years ago.
At a time when healthcare systems and access to care continue to evolve, I feel a strong sense of purpose in the work we do. Pediatric and adolescent gynecology allows us to make a meaningful difference early in our patients’ lives, promoting reproductive health, reducing disparities, and ensuring that young people receive the care and support they need to thrive. By collaborating with our MIGS colleagues, we continue to strengthen the care we provide and broaden access for the next generation of patients. Over the past few years we have developed relationships with AAGL clinicians with particular interest in hysteroscopy, endometriosis management, and innovative and new technology, and this is just the beginning! I have learned so much from members of AAGL, from how to edit a surgical video to best practices in documentation of endometriosis surgery. During times that may feel uncertain, I find reassurance and optimism in the collegiality of our professional community.
On behalf of our PAG SIG leadership, I welcome you to attend our World Congress of Pediatric and Adolescent Gynecology, held in the USA for the first time since 1986, April 23-25 in San Francisco, California. More information can be found at www.wcpag2026.com. With attendees from all over the world, we are sure that this conference will help continue to facilitate ongoing conversations and collaborations. Working together with purpose and compassion, we strengthen access to care, advance our science, and help build a healthier future for the next generation.
Lissa Yu, MD
Dr. Yu is the Chair of the AAGL Pediatric and Adolescent Gynecology Special Interest Group (SIG) and Assistant Professor of Pediatric and Adolescent Gynecology at Seattle Children’s Hospital and University of Washington School of Medicine Department of Obstetrics and Gynecology in Seattle, Washington.

SIG Recommended SurgeryU Video #1:
Laparoscopic Oophoropexy with Combined Fixation to Uterosacral Ligament and Pelvic Side Wall in a Prepubertal Girl With Recurrent Ovarian Torsion
Lissa Yu, MD, Whitney Wellenstein, MD, Tara Streich-Tilles, MD, Lesley Breech, MD
A seven-year-old girl underwent laparoscopic oophuropexy, a surgical procedure to prevent ovarian torsion, using both fixation to the utero-sacral ligament and the pelvic sidewall due to her age and anatomy. This video highlights the differences in anatomy noted in a prepubertal patient and addresses challenges and limitations of typical oophoropexy techniques due to these differences.
 Click Image to View Video
Click Image to View Video
SIG Recommended SurgeryU Video #2:
The Utililty of Endosee as a Bedside Vaginoscope in the Prepubertal Child
Madeline Ross, MD, Ashli Lawson, MD
This video reviews the use of the Endosee hysteroscopic device for evaluation of the vaginal cavity in a pediatric patient. This video demonstrates the use in both a post-pubertal and pre-pubertal patient and illustrates the utility of a vaginoscopy when a speculum cannot reasonably be utilized.

JMIG Article Recommendation #1:
Recurrent Ovarian Torsion: Risk Factors and Predictors for Outcome of Oophoropexy
Amir Akdam, MD, Nati Bor, MD, Yuval Fouks, MD, Maya Ram, MD, Ido Laskov, MD, Ishai Levin, MD, and Aviad Cohen, MD
This article highlights the diagnostic challenges of adnexal torsion in pediatric and adolescent patients, emphasizing that torsion frequently occurs in younger patients and those with normal-appearing ovaries and more commonly reoccurs in the absence of ovarian pathology. It also discusses the efficacy of oophoropexy, highlighting that there is no single fixation procedure that is superior. Finally, it underscores the importance of ovarian sparing detorsion regardless of ovarian appearance and urges gynecologists to adopt conservative surgical management to preserve future fertility in young patients.
JMIG Article Recommendation #2:
Obstructive Reproductive Tract Anomalies: A Review of Surgical Management
Bethany Skinner, MD, and Elisabeth H. Quint, MD
This article provides a framework for the evaluation and surgical management of obstructive Mullerian anomalies in adolescents. These are important as obstructive Mullerian anomalies that can cause significant pain and place patients at higher risk for endometriosis. It emphasizes the need for early diagnosis, thoughtful preoperative planning, and patient centered surgical decision making. Finally, this article calls on gynecologists to maintain familiarity with these rare, but impactful conditions to ensure accurate and timely management.
SurgeryU Video and JMIG Article Recommendations By:
Megan McCracken, MD

Dr. McCracken is a AAGL PAG SIG member and a Fellow of Pediatric and Adolescent Gynecology at Stanford University School of Medicine in Stanford, California.

Hysteroscopic Excision of Obstructive Sterine Septum in a Patient With Atypical Robert’s Uterus
A 12-year-old with a history of repaired rectoperineal fistula and left solitary kidney presented with progressive dysmenorrhea following menarche. Shortly after thelarche at age 10, surveillance pelvic ultrasound showed a bicornuate uterus. Vaginoscopy and hysteroscopy were performed: The vaginoscopy showed a single vaginal canal and single apical cervix. Subsequent hysteroscopy showed a single tubal ostium toward the patient’s left with no right sided cavity or tubal ostium visualized. The discrepancy between the ultrasound and examination findings raised suspicion for an obstructive Müllerian anomaly. The patient was closely monitored for pain and menarche.
Approximately 18 months later, she underwent menarche and experienced significant dysmenorrhea. Repeat pelvic ultrasound again showed a bicornuate uterus; pelvic MRI showed a left uterine horn communicating with a normal appearing cervix, in addition to a distended right uterine horn that did not communicate with the cervix (Figure 1). A septum was visualized between the two horns with thick muscular tissue near the fundus and thin fibrous tissue more caudally. A right hematosalpinx was also noted.
She was started on norethindrone acetate for menstrual suppression with plans to proceed with hysteroscopic septum resection under laparoscopic guidance, and she discontinued norethindrone acetate 6 weeks prior to her scheduled surgery to allow for re-accumulation of hematometra to aid in surgical resection. A vaginoscopy was first performed, again confirming a normal single vagina with a single apical cervix. On hysteroscopy she was again found to have a single uterine horn with a normal tubal ostium off to the patient’s left. There was no obvious bulge delineating the location of the thin fibrous septum, so a diagnostic laparoscopy was performed to confirm the anatomy. The laparoscopic light was turned off, and the hysteroscope was introduced into the uterine cavity again which identified the location of the obstructive uterine septum.
The resectoscope was then introduced into the uterine cavity and the uterine septum was incised under laparoscopic guidance. After entry of the obstructed cavity, a normal right tubal ostium was identified (Figure 2). Continued resection of the fibrous portion of the uterine septum occurred until the opening was sufficiently large. All port sites were closed with absorbable suture.
Conclusion:
A Robert’s uterus is a rare uterine anomaly usually involving a single uterine body with a dividing septum occluding one side of the uterus above the internal cervical os. In this case, we describe an atypical Robert’s uterus consisting of a combined bicornuate septate uterus divided by a septum occluding one side of the uterus above the internal cervical os. Given her known history of anorectal and renal anomalies, she underwent post-pubertal screening with ultrasound, allowing for prompt diagnosis of an obstructive Müllerian anomaly. There is no standard of care for surgical approach for patients with complex obstructive Mullerian anomalies. Septal resection can be quite challenging, especially when the uterine cavity is decompressed. Concurrent use of laparoscopic guidance helped delineate the septum location, as well as confirm location and direction of hysteroscopic excision to avoid uterine perforation or other intra-abdominal injury.
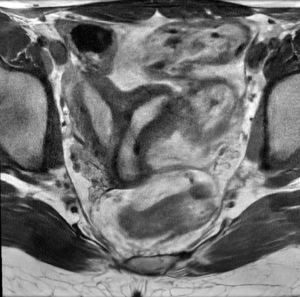
Figure 1: Pelvic MRI showing noncommunicating right uterine horn and normal communicating left uterine horn.
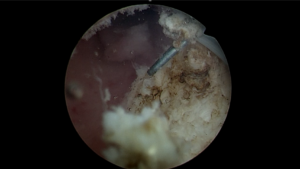
Figure 2: Resectoscope excision of fibrous septum with entry into the now visible right uterine horn.
References:
- Pfeifer SM, Attaran M, Goldstein J, Lindheim SR, Petrozza JC, Rackow BW, Siegelman E, Troiano R, Winter T, Zuckerman A, Ramaiah SD. ASRM müllerian anomalies classification 2021. Fertil Steril. 2021 Nov;116(5):1238-1252. doi: 10.1016/j.fertnstert.2021.09.025.
- de Beaufort CMC, Hooijer IN, Kuijper CF, Arguedas Flores OE, de Jong JR, van den Boogaard E, Dekker JJML, Gorter RR. Anatomical Gynecological Anomalies in Girls Born with Anorectal Malformations: A Retrospective Cohort Study of 128 Patients. J Pediatr Adolesc Gynecol. 2024 Feb;37(1):56-62.
- Gulino FA, Occhipinti S, Ettore C, Incognito GG, Russo E, Cannone FG, Ettore G. Challenges in the diagnosis and management of Robert’s uterus: Systematic review and case presentation. Journal of Clinical Ultrasound. 2024 Jun;52(5):619-28.
- John SK, Prabhu PS, Virmani S, Kumar V, Thotan SP. Misdiagnosed Roberts uterus leading to surgical misadventures. Journal of Pediatric and Adolescent Gynecology. 2017 Aug 1;30(4):508-10.
- Gao K, Zhang H, Zhu J, Yu M. Intrauterine adhesions combined with Robert’s uterus: a case report and literature review. Archives of Gynecology and Obstetrics. 2022 Oct;306(4):1069-75.
- Management of Acute Obstructive Uterovaginal Anomalies: ACOG Committee Opinion, Number 779. Obstet Gynecol. 2019 Jun;133(6):e363-e371.
About the Author:
Katherine Byrket, MD, and Y. Frances Fei, MD
Drs. Byrket and Fei are members of the AAGL Pediatric and Adolescent Gynecology SIG. Dr. Byrket is a Pediatric and Adolescent Gynecology Fellow at Nationwide Children’s Hospital in Columbus, Ohio. Dr. Fei is an Assistant Professor and Fellowship Program Director of Pediatric and Adolescent Gynecology at Nationwide Children’s Hospital and The Ohio State University Medical Center in Columbus, Ohio.

Artificial Intelligence in Pediatric and Adolescent Gynecologic Surgery: Opportunities and Challenges
Artificial intelligence has rapidly been reshaping surgical care. In Pediatric and Adolescent Gynecology (PAG), the patient population and the clinical scope make it a compelling space for thoughtfully designed AI tools that could personalize care and enhance clinical decision-making.
Preoperative Counseling
In the preoperative setting, large language models (LLMs) have the potential to meaningfully enhance counseling and support surgical decision-making. LLM-generated chatbot explanations of risks, benefits, and alternatives of six common surgical procedures have been rated as less complex and more complete than surgeon-generated informed consent materials1. One useful LLM model presently used is Dr. Momfidence from Girlology2. Preoperative counseling tools and chatbots can support developmentally appropriate surgical conversations for children and teens by tailoring language and information in an individualized way.
Diagnostic Imaging
3D modeling and virtual reality (VR) visualization of complex anomalies can improve counseling, trainee education, and surgical planning by reconstructing imaging into models to guide surgical approach3. There are currently no published studies examining machine learning and imaging characterization of Mullerian anomalies. With the wide range in complexity involved in these anomalies, large and diverse training datasets will be required to develop reliable models.
Intraoperative Guidance
In the operating room, machine learning applied to surgical videos has shown potential as a form of intraoperative guidance. In a recent systematic review spanning across surgical specialties4, AI models could identify specific procedural steps in surgical videos with accuracies ranging from 81% to 93.2%, and could successfully recognize relevant anatomy with accuracies between 71.4% and 98.1%. Performance depends on the size of training data sets and their quality, and a known limitation is that pediatric data has not been routinely used in training data sets. In PAG, the need for more robust data sets to train intraoperative AI tools is driven in part by challenges of complex anomalies and age-related anatomic variation (such as the small prepubertal uterus).
Surgical Training
AI is revolutionizing surgical training through the use of enhanced tools such as virtual simulations, real time feedback and skills assessment5. AI enhances the opportunities for remote surgical training so experts can mentor trainees in real time across vast distances, an invaluable opportunity for those who may not have access to a local PAG specialist.
Privacy and Safety
Alongside these technical opportunities, attention to privacy and safety in the pediatric space remains essential. The American College of Obstetricians and Gynecologists, in line with professional pediatrics organizations, underlines that confidential care for teens promotes trust in their provider and encourages patient engagement in their own care6. Having access to age-appropriate LLM-based chatbots specifically created for children and teens can be a way for explanations to feel more accessible7. Safeguarding will require thoughtful data infrastructure, meaningful patient and parental consent processes, and preemptive protocols for moments of disagreement between children, parents, and healthcare providers7.
Conclusion
AI systems hold promise for transforming preoperative counseling, diagnostic precision, and intraoperative support in PAG. With intentional investment in pediatric datasets and responsible governance, AI can become a powerful tool in delivering quality surgical care for young patients.
References
- Decker H, Trang K, Ramirez J, et al. Large Language Model−Based Chatbot vs Surgeon-Generated Informed Consent Documentation for Common Procedures. JAMA Netw Open. 2023;6(10):e2336997. doi:10.1001/jamanetworkopen.2023.36997
- Girlology, Inc. » Get Momfidence. June 11, 2024. Accessed February 6, 2026. https://girlology.com/get-momfidence/
- From A, Dumont T, Singh S, Duigenan S, Flaxman T. Navigating Complexity: Advanced Visualization for Müllerian Anomalies and its Implications for Diagnoses and Surgical Planning. J Pediatr Adolesc Gynecol. 2025;38(6):747-749. doi:10.1016/j.jpag.2025.06.005
- Paracchini S, Taliento C, Pellecchia G, et al. Artificial intelligence in the operating room: A systematic review of AI models for surgical phase, instruments and anatomical structure identification. Acta Obstet Gynecol Scand. 2025;104(11):2054-2064. doi:10.1111/aogs.70045
- Kewalramani D, Jawa RS, Martin CA, et al. Position statement from the society of University surgeons, surgical education committee: Artificial intelligence in surgical training for medical students, residents, and fellows. Surgery. 2026;190. doi:10.1016/j.surg.2025.109849
- Confidentiality in Adolescent Health Care: ACOG Committee Opinion, Number 803. Obstet Gynecol. 2020;135(4):e171-e177. doi:10.1097/AOG.0000000000003770
- Allen JW, Earp BD, Wilkinson D. AI-assisted consent in pediatric medicine: ethical implications of using large language models to support decision-making. J Med Ethics. Published online August 6, 2025. doi:10.1136/jme-2024-110624
About the Authors:
Olga Kciuk, Clinical Assistant Professor
Nichole Tyson, Clinical Professor


Dr. Kciuk is Clinical Assistant Professor of Pediatric and Adolescent Gynecology at Stanford University in Stanford, California. Dr. Tyson is Division Chief and Clinical Professor of Pediatric and Adolescent Gynecology at Stanford University in Stanford, California