Spotlight On: Hysteroscopy / Intrauterine Surgery


This month, we cast a spotlight on articles, SurgeryU videos, and Journal of Minimally Invasive Gynecology (JMIG) article recommendations from the AAGL Hysteroscopy / Intrauterine Surgery (SIG) led by Chair, Jovana Tavcar, MD.
Access to SurgeryU and JMIG are two of the many benefits included in AAGL membership. The SurgeryU library features high-definition surgical videos by experts from around the world. JMIG presents cutting-edge, peer-reviewed research, clinical opinions, and case report articles by the brightest minds in gynecologic surgery.
SurgeryU video and JMIG article recommendations by our SIGs are accessible by AAGL members only. For full access to SurgeryU, JMIG, CME programming, and member-only discounts on meetings, join AAGL today!

SIG Recommended SurgeryU Video #1:
Microcolpohysteroscopy
By Alka Kumar, MD, Luigi Montevecchi, MD
This video highlights a specialized technique combining colposcopy and hysteroscopy to provide magnified in vivo visualization of the cervix and endometrium which can be used in the diagnosis and management of various gynecologic conditions. It is an important technique exploring how cellular examination can be conducted with hysteroscopy.
 Click Image to View Video
Click Image to View Video
SIG Recommended SurgeryU Video #2:
Office Equipment Set-Up & How to Use it
By Jovana Tavcar, MD, Christina Salazar, MD, Erica Robinson, MD, Stephanie Morris, MD
This video, originally presented as a postgraduate course at AAGL, is a practical guide regarding indications, set-up, technique, and clinical pearls for the performance of hysteroscopy in an outpatient office setting. It provides highly useful information for any gynecologist looking to set-up or expand their practice of office hysteroscopy – which can improve treatment efficiency and reduce cost for both patients and hospital systems
Aparna Ramanathan, MD, MPH

Dr. Ramanathan is a member of the AAGL Hysteroscopy / Intrauterine Surgery SIG and a MIG Surgeon at the University of Washington Medical Center in Seattle, Washington.

JMIG Article Recommendation #1:
Surgical Management of Early Pregnancy Loss by Operative Hysteroscopy vs Vacuum Aspiration: Short-Term Outcomes of a Randomized Controlled Trial
Maya Naor-Dovev, MD, Boris Beloshevski, MD, Mata Mor, MD, Hila Segal, MD, Neta Eisenberg, MD, Noam Smorgick, MD
This is a randomized controlled trial comparing management of early pregnancy loss by vacuum aspiration vs operative hysteroscopy for the primary outcome being rates of IUA in the two groups. The rates of IUA were significantly higher after the vacuum aspiration (19/42 cases, 45.2%) compared with the operative hysteroscopy (2/48 cases, 4.2%) (p < .01). While the current evidence does not support replacing vacuum aspiration with HSC removal of RPOC for all patients. it may be suitable for selected patients who are at risk for IUA, such as those with history of IUA or recurrent pregnancy loss.
JMIG Article Recommendation #2:
Incidence of Intrauterine Adhesions After Myomectomy and Association With Intraoperative Entry of the Endometrial Cavity
Sweta Ghatti, BA, Gwendolyn Towers, MD, Mindy Pike, PhD, Nicholas Hazen, MD, James K. Robinson, III, MD, MS, Aparna Ramanathan, MD, MPH
This article shows the incidence of intrauterine adhesions after different types of myomectomy, evaluated by office hysteroscopy three months postoperatively. High incidence of 17.4% of intrauterine adhesions post myomectomy, underscores the importance of offering postoperative office hysteroscopy, particularly in patients desiring future fertility, even more so in cases of intraoperative entry in the uterine cavity.
JMIG Articles Recommendations By:
Jovana Tavcar, MD
Dr. Tavcar is Chair of AAGL Special Interest Group in Hysteroscopy and Intrauterine Surgery and attending physician and Assistant Professor of OBGYN at Medstar Georgetown University Hospital, in Washington DC.

Mullerian Papilloma of the Uterine Cervix in a 3-Year-Old Girl: The Importance of Vaginoscopy
Mullerian papilloma is a rare benign pleomorphic tumor of the cervix with unclear prevalence, as documented cases in the literature are limited. This epithelial neoplasm arises from mullerian epithelium, which is of embryological origin and develops from remnants of the fusion of the paramesonephric ducts. It has a distinct histological and immunohistochemical profile and typically shows low potential for malignancy. These tumors are more commonly found in girls and are rarely seen in adult women. They can present as papillomatous or exophytic lesions on the cervix, often asymptomatic, but may sometimes cause intermittent genital bleeding prior to menarche.
Due to their hidden nature in routine physical examinations and the limited sensitivity of imaging studies like gynecological ultrasound for diagnosis, endoscopic vaginoscopy emerges as a crucial diagnostic and therapeutic tool.
Case Presentation: A 3-year-old girl with normal development presented cyclical, self-limited, scant bleeding lasting five months. She showed no signs of secondary sexual characteristics or vulvoperineal lesions. The diagnostic workup included a normal prepubertal hormonal profile, gynecological ultrasound, and pelvic radiographs.
Operative hysteroscopy was conducted for diagnosis. This inpatient procedure required sedation. A vaginoscopic approach using a 30° optic lens from a Bettocchi set was employed and during the procedure, a 2 cm friable polypoid cervical lesion was identified and excised using a 5Fr grasper (See image 1 and 2). Histopathological examination indicated that the tumor comprised papillary excrescences lined by mucosecretory epithelium, supported by dense fibrous stroma with spindle-shaped and stellate fibroblasts. Immunohistochemistry for myogenin and desmin was negative.
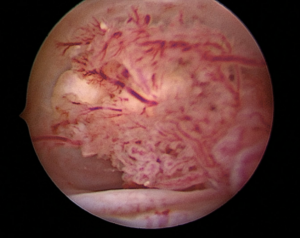
Image 1
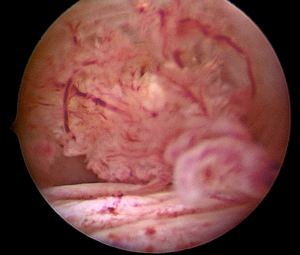
Image 2
The macroscopic appearance of mullerian papilloma can easily be mistaken for malignant tumors, particularly vaginal rhabdomyosarcoma, due to its vascularized papillae that may resemble atypical vessels. Treatment involves excising the lesion.
Vaginal assessment and direct visualization are essential for diagnosing patients exhibiting genital bleeding or persistent pathological discharge (See image 3). While small “virginal” specula are available, they can cause discomfort and convey negative psycho-sexual effects on girls and adolescents. Vaginoscopy offers a superior method for assessing intravaginal pathology and diagnosing intravaginal foreign bodies. It is best performed with a hysteroscope equipped with a working channel, such as the Bettocchi set, facilitating diagnosis confirmation and treatment, as seen in our patient.

Image 3
With a caliber of less than 5mm, the procedure is performed gently without the need for specula or blades. Using saline or distilled water for distention provides clear visibility even in cases of scant active bleeding or vaginal discharge, allowing comprehensive visualization of the vaginal canal, cervical integrity, and exploration of the endocervical canal if necessary.
Although this procedure can be done in an office setting without anesthesia and is well tolerated by adults, sedation may be preferable for girls to reduce anxiety and increase cooperation. In conclusion, vaginoscopy enables complete visualization of the vaginal canal and cervix, making it the examination of choice when vaginal or cervical pathology is suspected, thus facilitating diagnosis, biopsy, and often treatment in a single encounter in a “see & treat” approach.
About the Authors:
Mariana Boutmy, MD
Valeria Bentancor, MD
Rosina Pisón, MD



Drs. Boutmy, Bentancor and Pisón are staff of the Hysteroscopy Unity at British Hospital in Montevideo, Uruguay.

The Next Era of Hysteroscopy: Miniaturized, Intelligent, Sustainable
Office hysteroscopy has progressively displaced operating room-based procedures as the preferred first-line approach for evaluating and managing intrauterine pathology, a transition underpinned by incremental advances in optics, instrument miniaturization, and fluid management engineering rather than any single disruptive breakthrough. Contemporary ambulatory systems now permit direct endometrial cavity visualization in women presenting with abnormal uterine bleeding (AUB), infertility, recurrent pregnancy loss (RPL), or suspected intrauterine adhesions, and allow targeted biopsy within the same encounter, achieving a diagnostic yield that general anesthesia–dependent protocols historically struggled to match while imposing substantially greater procedural burden on both patients and healthcare systems. (1)
A particularly consequential hardware development has been the emergence of reposable, handheld hysteroscopic platforms that pair a reusable electronic display processor unit with disposable, single-patient cannulas incorporating a micro-camera, integral light source, and distension channel. These cordless, lightweight devices can be deployed within a standard examination room without dedicated endoscopy infrastructure, which meaningfully lowers the adoption threshold for practices lacking legacy tower-based equipment and raises realistic prospects for implementation in resource-constrained environments. (2) A prospective cohort comparing one such handheld device against a conventional 2.9-mm rigid office hysteroscope demonstrated procedural adequacy, histopathological concordance with operating room specimens, and patient-reported pain scores that were statistically non-inferior. Although encouraging, the single-center design, operator familiarity bias, and relatively modest sample size limit generalizability and warrant confirmation through adequately powered, multicenter trials. (3)
Parallel innovation has extended the ambulatory remit beyond diagnosis toward operative management. Fully single-use, battery-powered operative hysteroscopes, featuring slim rigid catheters with steerable distal tips, dual inflow and outflow channels, and working channels compatible with disposable forceps, scissors, and snares, have been evaluated in outpatient procedure rooms for polypectomy, removal of retained products of conception (RPOC), and carefully selected submucous fibroids. (4) Feasibility data from a multicenter pilot series reported acceptable visualization quality and physician-rated performance, though the abstract-level evidence base, absence of comparative controls, and short follow-up preclude any conclusions about efficacy equivalence to conventional resectoscopic approaches. The elimination of reprocessing cycles addresses legitimate concerns about cross-contamination and workflow disruption. However, the per-procedure cost differential, environmental burden of disposable polymer instrumentation, and long-term sustainability implications require explicit cost-effectiveness analysis before widespread adoption can be responsibly endorsed. (5)
Digital adjuncts, particularly deep-learning models trained on annotated hysteroscopic image datasets, have achieved promising intrauterine lesion detection and classification accuracy in retrospective studies, with reported performance metrics comparable to experienced operators for discrete pathology categories. (6) Critical limitations persist nonetheless. Existing datasets reflect referral center case-mix distributions that may not represent community practice, most models lack external validation on ethnically and clinically diverse populations, and prospective integration into live hysteroscopic workflows remains largely uncharted. Alongside these technological trajectories, consensus statements have reinforced the primacy of standardized terminology, structured competency-based training, and evidence-based pain-minimizing techniques, including the vaginoscopic approach, small-caliber instrumentation, and optimized distension pressure, as prerequisites for safe dissemination of any new platform. (7) Future research must prioritize rigorous comparative effectiveness trials, real-world implementation studies in low-resource settings, and prospectively validated AI diagnostic pipelines before these technologies transition from promising innovation to evidence-based clinical standards.
References:
- De Silva PM, Smith PP, Cooper NAM, Clark TJ. Outpatient hysteroscopy (Green-top Guideline No. 59). BJOG. 2024;131(13):e1–e19.
- Okohue JE, Okohue JO. Establishing a low-budget hysteroscopy unit in a resource-poor setting. Gynecol Minim Invasive Ther. 2020;9(1):18–23.
- Carlson MJ, Kidrowski C, Bain K, Garg B, Patel B, Memon H. Diagnostic office hysteroscopy with the Storz TrophyScope® versus Cooper Surgical Endosee®. Minerva Ginecol. 2020;72(5):310–315.
- Althoff K, et al. LiNA OperaScope: pilot evaluation of a single-use operative hysteroscopy system [abstract]. J Minim Invasive Gynecol. 2020;27(Suppl):S231.
- Pioche M, Pohl H, Cunha Neves JA, et al. Environmental impact of single-use versus reusable gastroscopes. Gut. 2024;73(11):1816–1823.
- Raimondo D, Raffone A, Salucci P, et al. Detection and classification of hysteroscopic images using deep learning. Cancers (Basel). 2024;16(7):1315.
- Carugno J, Grimbizis G, Franchini M, et al. International consensus statement for recommended terminology describing hysteroscopic procedures. J Minim Invasive Gynecol. 2022;29(3):385–391.
About the Authors:
Alka Kumar, MD
Adel Sedrati, MD
 Dr. Kumar is a member of the AAGL Hysteroscopy and Intrauterine SIG and the AAGL Board of Directors and is Director of the Women’s Health Centre in Jaipur, Rajasthan, India.
Dr. Kumar is a member of the AAGL Hysteroscopy and Intrauterine SIG and the AAGL Board of Directors and is Director of the Women’s Health Centre in Jaipur, Rajasthan, India.

Dr. Sedrati is a member of the AAGL Hysteroscopy and Intrauterine SIG and a MIG Surgeon and Director of the Office Hysteroscopy Center of Excellence in Constantine, Algeria.